My research activities as a part of PersonalizeAF team mainly focus on detection and localization of regions in atria exhibiting some specific types of electrical activities or conduction patterns as we call them. We aim to develop computational tools that can robustly pinpoint these regions. This localization can help us have a better understanding of atrial fibrillation (AF) and also guide physicians to additional ablation targets in cases where common ablation strategies do not work. I would like to start my series of blogs which will concentrate of local AF driver detection techniques ablation strategies.
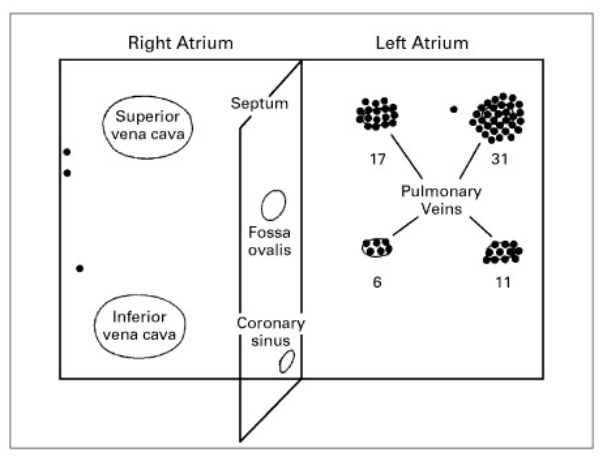
In 1998, Haïssaguerre and his team first reported that the pulmonary vein ectopy might be the trigger of AF. In 45 patients they evaluated, 94% of all ectopic sites were located in the vicinity of pulmonary veins (see Fig. 1). Then the electrical isolation of this region, a therapy called as Pulmonary Vein Isolation (PVI), could eliminate AF. The team has performed radio frequency ablation on 38 of these patients and by the end of 7 months follow-up, 62% had no AF episodes without any drug therapy. This was a promising step and the start of the “era of non-pharmacologic AF therapies” [2].