The human body gets atrial cells through self organization. During embryo development cells continuously secrete factors to their surroundings. Because of the differing positions of each cell (for example at the edge of the embryonic body or its core) a “gradient”” or differing concentration of these factors in the different sections of the embryo is created (for example more of a factor at the center of a cell group). As cells experience distinct signals due to these deviating concentrations, the result is them differentiating into various cell types, like our heart muscle cells.
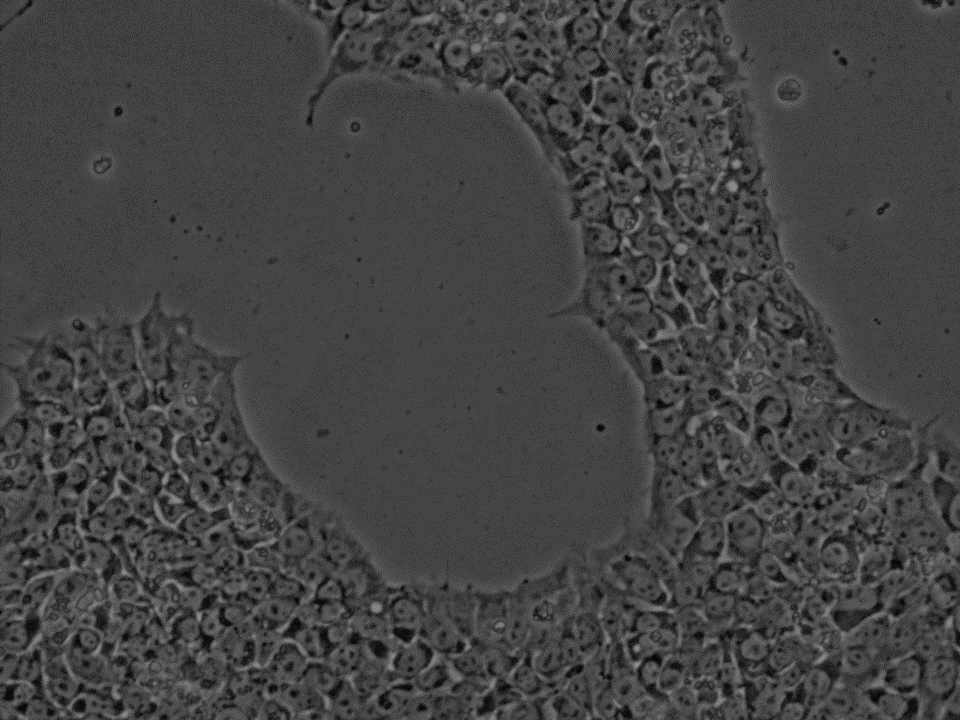
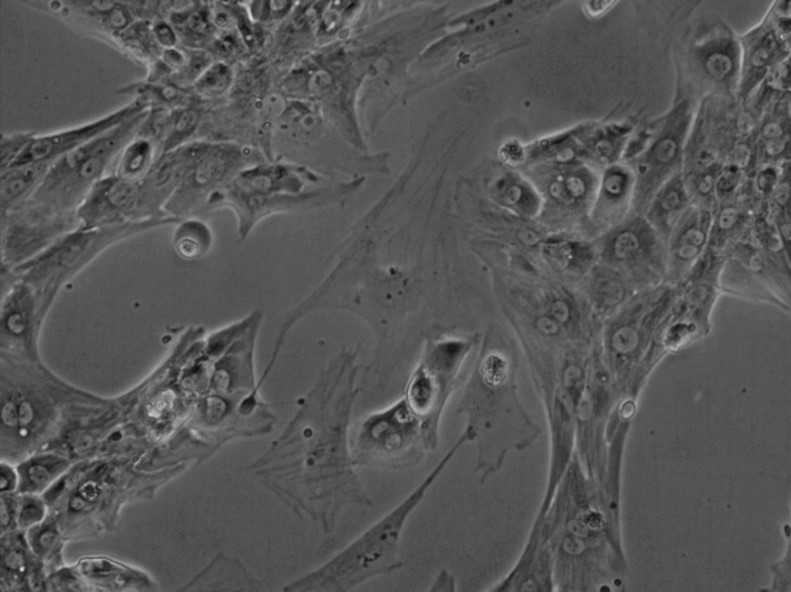
Using these native atrial heart muscle cells of a patient in the lab to study disease is however difficult, as their extraction could be harmful and they cannot be maintained in the lab for a long time. Therefore utilizing induced pluripotent stem cells and instead differentiating them into atrial cells has been a promising approach. By mimicking the natural process in the embryo through the use of proteins or small molecules, signaling pathways that cause the specification into certain cells can be activated. This process has to be tailor-made for each cell type as we need to work with the natural programming of a cell to let it become a specific type while suppressing the normal tendency of pluripotent stem cells to differentiated into various cells types.
For heart cells this is done by manipulating the “Wnt” signaling pathway. By activating and deactivating it, pluripotent stem cells are first nudged into becoming mesoderm cells and subsequently cardiomyocytes (heart muscle cells). This has so far been usually applied to produce ventricular cardiomyocytes, but through the addition of retinoic acid atrial muscle cells could also be differentiated already. If you want some more detail check out this link explaining Wnt signalling for heart muscle differentiation, it goes into specifics but it is worth a look to just have an idea of what your cardiomyocytes have been through to get where they are.