So here we are with tissue under highly controlled mechanical environment. Atria are not functionally required to produce as much force and in normal condition their peak of contraction has lower amplitude compared to ventricles. However, to better understand the difference between atrial and ventricular contractile behavior, it is possible to increase force generation via drug stimulation.
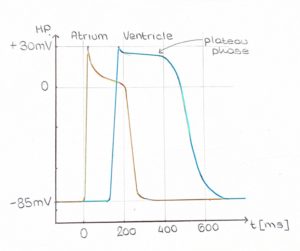
From the electrophysiological perspective, atria are characterized by a shorter action potential (AP), with a non-so-flat plateau phase (Figure 1). As you may already now, heart contraction is initiated by electrical stimuli, therefore it is not surprising that this difference in AP shape results in a different contraction waveform. Due to their different electrophysiological properties, atrial tissue has a steeper and almost instantaneous peak (Figure 2, yellow trace), whereas ventricular tissue has clearly distinguishable contraction and relaxation slopes (green trace).