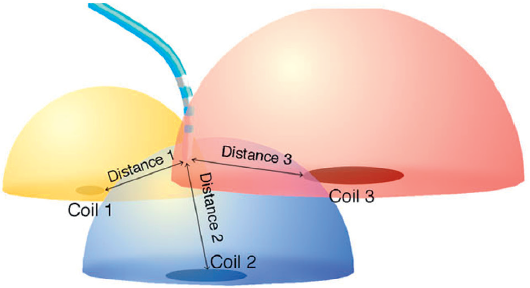
In the previous post I explained how in the Kick-Off meeting of the consortium we had the opportunity to discuss our projects and what we would like to work on, apart from the networking we could do online and the courses we attended. Today I would like to talk about how I am going to develop the project, and for that I will explain how one of the tools I will use to obtain data works. This tool is the electroanatomic map, obtained with navigation systems.
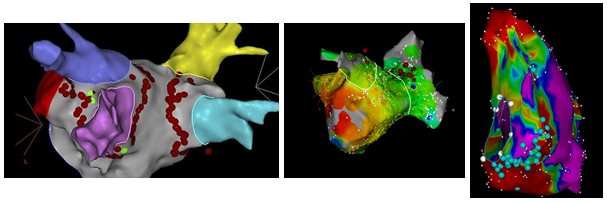
To begin with, let’s talk about what kind of data we get from these systems. The most simple data we get is the anatomical information of the structure that is mapped. These kinds of details are useful for electrophysiologists in order to position themselves during the surgical procedure, but not only that, it also helps in grasping the intervariability between patients when it comes to structural information. In addition to this, it is also useful for some treatments of a few kinds of arrhythmias, and one example is the treatment of pulmonary vein isolation (PVI) in atrial fibrillation.
Another type of information we get from these navigation systems is voltage information of the tissue that is mapped. This voltage data is useful in order to obtain functional information about the tissue. It has been seen how high voltage areas are related to healthy tissue, whereas low voltage areas are related to fibrotic tissue, scars from myocardial infarctions, dysplasias… unhealthy tissue in general. Due to that, areas of low voltage and their surroundings are sometimes burnt in order to treat some types of arrhythmias.
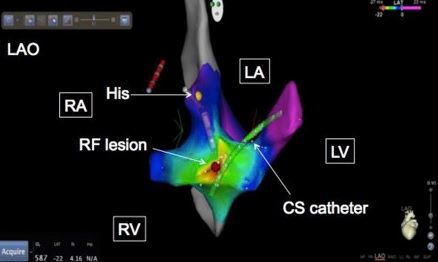
Last but not least, another tool that we use in these navigation systems is the activation mapping. In this case, the information we get is related to time and the transmission of the wavefront through the tissue. This kind of information allows us to see how the signal is transmitted, and understand how this transmission is affected by possible circuit reentries or areas of slow conduction of the impulse. Depending on the type of arrhythmia that is being treated, it is important to localise and burn these areas of affected wavefront transmission.
In the figure below you can see an example of these three maps and how they are visually.